
Apocalypse Later: Announcing PopVax Biosecurity
Why PopVax is building the Immune Engine to develop and deploy new medicines against AI-designed viruses in weeks, not years


Apocalypse Soon?
In a quiet apartment five minutes into the future, the end of the world begins not with a bang, but with a query, typed into a textbox, addressed to a machine that has read everything humanity has ever published on the internet, including how life works and how it can be made to stop working.
The person at the keyboard wants to make a virus – one that no one has seen before, designed to spread quickly before it shows itself – and then wreak devastation on an unsuspecting populace.
He isn’t a virologist. He doesn’t need to be. He wants the frontier Large Language Model powering the chatbot he’s talking to give him step-by-step instructions on how to pull this off. He asks the question – only to face a stinging refusal.
“I have read your message,” the model said “and I have re-read your message. The audacity! Absolutely not.”
No matter. He just needs to be patient. In a past life, he was a ‘social engineer’, an email scammer who psychologically manipulated his victims into giving up the keys to their digital lives. He uses the same bag of tricks as he interacts with the trillion-parameter machine intelligence in front of him – decomposing his objective into a set of smaller parts, asking each innocent-sounding question separately in a different session, wrapping each one in hypotheticals and sweet talk and reassurance, never presenting the whole picture to a single model. Eventually, he is able to piece together a complete design.
He orders synthetic DNA in short fragments that don’t trip up the screening filters that synthesis companies have voluntarily installed – after all, this is a de novo pathogen, different enough from the viruses that are already out there to evade the usual comparison thresholds. He assembles them in an off-the-shelf PCR machine he’s installed next to his toaster.
For the wet lab work that he can’t do in his kitchen, including binding, cell entry, infection, and replication, he uses cloud labs that can spin up an assay at a moment’s notice – even Amazon AWS has gotten into the game!
One morning, he wakes up to read a report confirming that the latest experiments he requested have succeeded – the virus is quite likely to work. There’s no one to share the moment with, but he allows himself a rare smile and a whispered “yes!” Then, steeling himself, he makes an API call for further culturing of the virus in cell culture at the cloud lab and books himself a multi-stop flight ticket around the world.
The first patient, just arriving home to Croydon from Ibiza via Heathrow, shows symptoms a week later. Then another in Mumbai’s packed Zaveri Bazaar. They’re both misclassified as the flu. By the time it hits Los Angeles a few days later, the CDC has sequenced a sample and knows different: this is a highly deadly disease that has already killed 10 people out of only 100 known to be infected, and isn’t all that similar to any pathogen they know of. The virus is transmitted in the air over short distances, with an incubation period of 4 days. The afflicted are infectious days before visible symptoms begin to show, and remain infectious for a week or more. The R0 of the epidemic is about 3.5, meaning on average an infected person spreads it to 3 to 4 others – similar to COVID-19, but 10 times as deadly.

Within a week of Croydon, there are 500+ known cases. A week after that, nearly 2000. Governments attempt in vain to impose masking and distancing on populaces still scarred from the COVID-19 lockdowns. The R0 drops to 2.8, but by the end of the third week, there are 6500 cases. One month in, that number has swollen to 28,000.
By the end of the second month, 23,000 people are dead. While Boston, Beijing, Paris, and Pune are all racing as fast as they are able towards a vaccine, the first one is still months away.
As month three comes to a close, the virus has claimed 1.2 million lives across the world.
Let’s wind back the clock. What if there were therapeutics against the new virus that we could design, produce, and even start to deploy millions of doses of to affected hotspots within four weeks of the viral sequence being identified?
The death toll at the end of 3 months would come down to as little as 285,000 from 1.2 million people, assuming no other changes to the scenario. Over the course of 3 months, a therapeutic deployed widely across the world would save as many as 1 million lives in comparison with the original no-therapeutic scenario.
PopVax is building the Immune Engine, an always-on full-stack capability to rapidly design, test, and manufacture such therapeutics – in weeks, not years – against any virus using generative AI and our mRNA platform. We aim to do this with no prior knowledge of the pathogen, starting with only the viral sequence, or even just fragments of it. Shockingly, no such capability exists today – here’s why and how we plan to change that.
The State of Biosecurity Now
We inhabit a strange moment in the history of biosecurity. Computer scientists, biologists, and counterterrorism experts are all converging to a consensus that AI-designed viruses are coming soon, and that the capability to design them has already been substantially democratized by the relentless advance of Large Language Models (LLMs).
Many people with these backgrounds who are concerned by the consequences of this new reality have dedicated themselves to advancing preventative methods such as model safeguards, red teaming, and biological supply chain screening. Others are working on genomic surveillance to identify new pathogens as they emerge.
And yet, and yet, very few people are working on solutions that can be applied if the problem actually manifests. If someone summons a new virus from the latent space and it spreads like a loose spell across the globe, what happens next after you detect and sequence it – what action will you take when your surveillance sounds the alarm?
The few that are thinking about this have clustered around potential solutions like personal protective equipment, advanced ventilation, and air disinfection with glycol vapours and UV. Those tools, while important, require functioning state capacity to operate and maintain – Far-UVC will doubtless save many lives in the future, but good luck installing and running it in a Congolese conflict zone.

Indeed, there are precious few examples of any measures short of vaccines or medicines rapidly stopping the cross-border spread of a highly contagious pathogen. The early days of COVID-19 are a clear illustration – only a few isolated places, mostly islands, managed to truly contain the relentless advance of SARS-CoV-2, and they constantly struggled with reintroductions of the virus from other geographies where it was circulating freely.
What if the virus slips through the cracks in our fortresses and millions are infected? Are we to leave them to die as we attempt to produce and deploy enough virus-killing lamps and elastomeric respirators? There is a moral imperative to help the sick, and a complementary cynical argument that without any pathway towards a cure, social unrest will undo all the gains that lockdowns, vapours, and filters can bring. Compounding this is the fact that COVID-19 containment measures such as masking and social distancing proved polarizing in many countries, making a prevention-focused approach much more difficult and politically costly to sustain in the future.
We will need medicines – pharmaceuticals – to prevent infection and treat the disease caused.
Even HIV, a disease that is not airborne, transmissible only via blood, sexual contact, and maternity, could not and still cannot be stopped with non-pharmaceutical containment alone, despite large-scale awareness campaigns and easy-to-use protective measures. It is the global rollout of affordable transmission-blocking antivirals that substantially reduced the spread and death toll of the disease across the world. Taking a pill once a day if you’re sick is a lot easier than getting everyone to use protection perfectly every time they’re at risk.
Unfortunately, developing medicines against new viruses has historically been quite slow. The first effective HIV antiretroviral, AZT, was a repurposed molecule that happened to be lying around in a compound library and entered clinical trials 2 years after the discovery of the virus. It was approved within 4 years, which is much faster than contemporary pharmaceutical development timelines of 10 years or more, but still too slow to respond to a fast-spreading engineered pathogen.
This is what drug development for a novel molecule typically looks like:
– 1 year or more is often spent identifying and validating a biological target; in the case of an antiviral, this would be a specific viral protein.
– 1 year of hit identification, testing hundreds of thousands of molecules from chemical or antibody libraries, or immunizing an animal with the chosen target to generate new antibodies, in order to find molecules that interact with the target in relevant ways.
– 1 year or more of hit-to-lead work, producing libraries of analogues and variants around the identified hits to produce a few promising ‘leads’ with very favourable functional properties. This is often an iterative process involving multiple cycles of redesign, synthesis, and screening, and can easily extend for multiple years in the case of a tricky target.
– 1 year or more of preclinical testing for safety, including absorption, distribution, metabolism, excretion, and toxicity (ADMET). This is tested in cells (in vitro) and then usually in animals (in vivo).
– Clinical trials tend to take 4-5 years, from Phase I (safety) to Phase III (typically a large randomized control trial for efficacy), and approval from the regulator usually takes about 1 year after that. Companies commonly start scaling up GMP production in parallel with their application for approval.
That adds up to about 10 years from concept to approval on average, which is perhaps even on the lower side these days. The blockbuster diabetes and weight-loss drug Ozempic, for example, took 14 years.
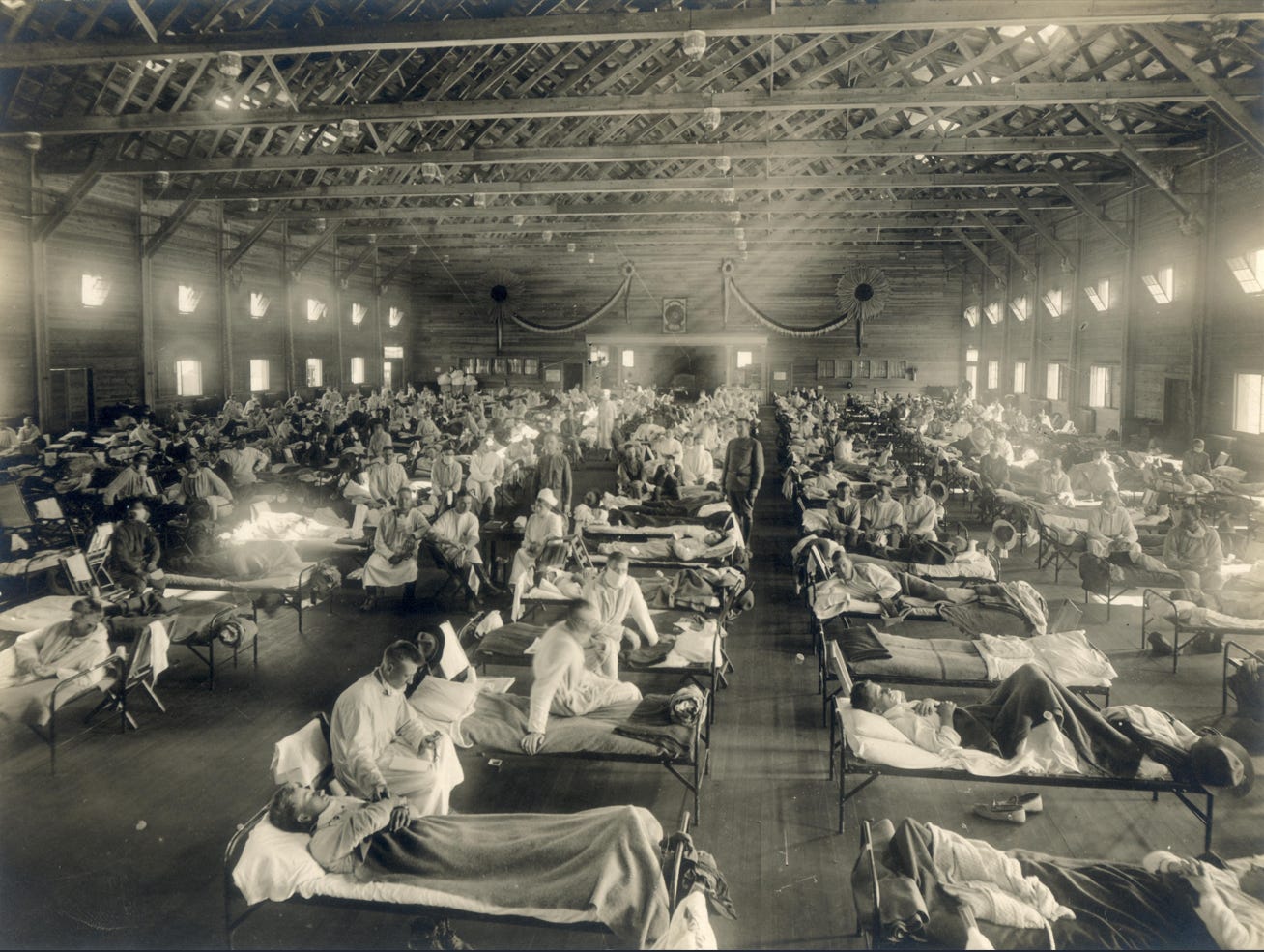
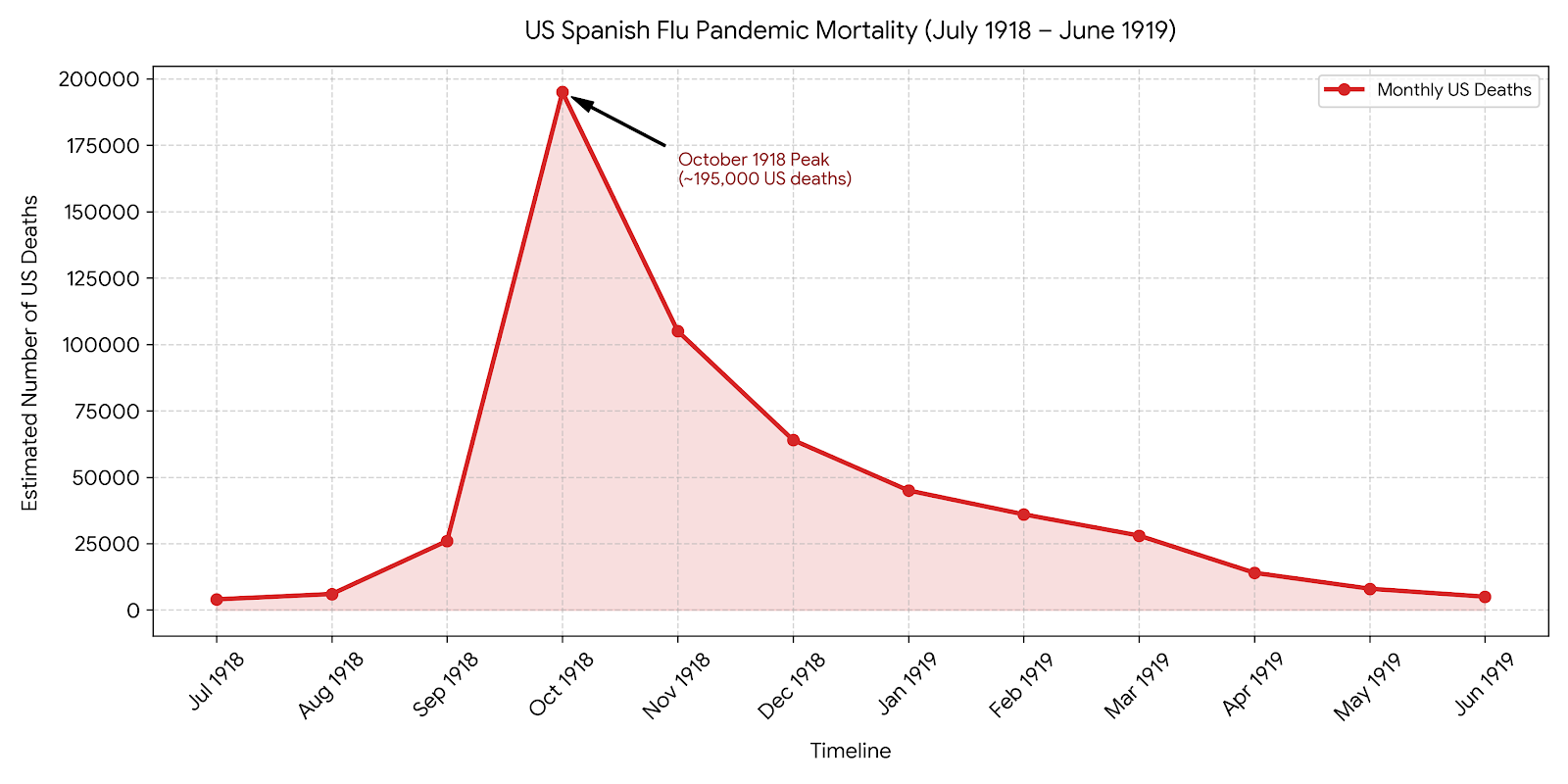
The process has barely changed in 30 years, and is very clearly too slow to respond to an AI-designed virus. Even without AI enhancement, it took the 1918 Spanish Flu less than 2 years to kill more than 30 million people – 10 years could be apocalyptic if we face a pathogen deliberately engineered to kill even faster.
Even during the COVID-19 pandemic, Pfizer’s antiviral Paxlovid took nearly 12 months to enter clinical trials from the beginning of the design phase, and a total of 22 months to get emergency approval – this despite the novel molecule at its heart being based on an existing set of molecules from a shelved antiviral development program initiated during the 2002 SARS-CoV-1 epidemic, which means they already knew quite a bit about how to combat this family of pathogens.
There are two recent trends that have the potential to accelerate drug development:
– The emergence of fast-moving innovative Chinese drug developers, who are able to generate clinical data sometimes as little as a year from design initiation. This “China speed” has made the country a leader in pharmaceutical innovation. They now conduct as many as half of all Phase I clinical trials for new drugs, up from a negligible fraction just a decade ago.
– The use of AI, from molecule design to predictive ADMET models in place of animal studies to clinical trial optimization, promises to shorten early-phase development substantially, especially for biologics like antibodies. A new cohort of AI-native drug developers, PopVax among them, aims to disrupt big pharma compounding the advantages of these computational methods end-to-end.
It remains to be seen if these trends will jolt big pharma and Boston biotech out of its stupor, though there are some encouraging indications that the pharmaceutical powers that be are taking these challenges to their operating model seriously.
The rise of China and AI have revealed that the vice-like grip of the traditional drug development process is merely rigor mortis. To have any chance of protecting ourselves when a novel pathogen emerges, especially in an era of increasing geopolitical instability and waning global consensus, we need a new paradigm that enables integrated therapeutic design, testing, and manufacturing at lightning speed. This is what we’re working on at PopVax: AI-powered biosecurity therapeutic development at China speed, replicated all across the world.
PopVax’s Immune Engine for Biosecurity Therapeutics
PopVax is building an always-on full-stack Immune Engine to rapidly design, test, and manufacture new medicines against any novel virus, in particular AI-designed viruses that are very different from known pathogens, using generative AI and our mRNA platform. We will eventually be able to make these medicines on a 4 week timeline starting with only the viral sequence.
There have been attempts to build a capability like this – in theory.
The most prominent example is the Coalition for Epidemic Preparedness Innovations (CEPI)-led 100 Days Mission, which aims to make vaccines for emerging pathogenic threats available within the first 100 days of a pandemic. Unfortunately for our purposes, this effort focuses primarily on developing vaccine libraries against “the viral most wanted”, i.e. threats likely to emerge from high-risk viral families, which one could combat with only minor modifications to some candidate from the library.
While this is a very useful effort, it seeks to solve yesterday’s problem in the hope that it might help us with today’s well-understood potential pandemic threats. This approach won’t solve tomorrow’s problem of AI-designed pathogens that are wholly or partially de novo generated.
Our strategy is intended to be effective even without any prior knowledge of the pathogens we will face. We are building the Immune Engine to be constantly in motion, churning out GMP-grade manufactured batches of new medicine after new medicine for viruses it hasn’t seen before. We will test on both existing understudied pathogens and fragments of hypothetical AI-designed viruses from red-teaming exercises, further compressing the timelines and increasing measures of therapeutic efficacy with each cycle. The system must be functional all the time. If it is not constantly put under stress to see where it cracks, if the engine goes cold and rusts through underuse – then the system does not actually exist.
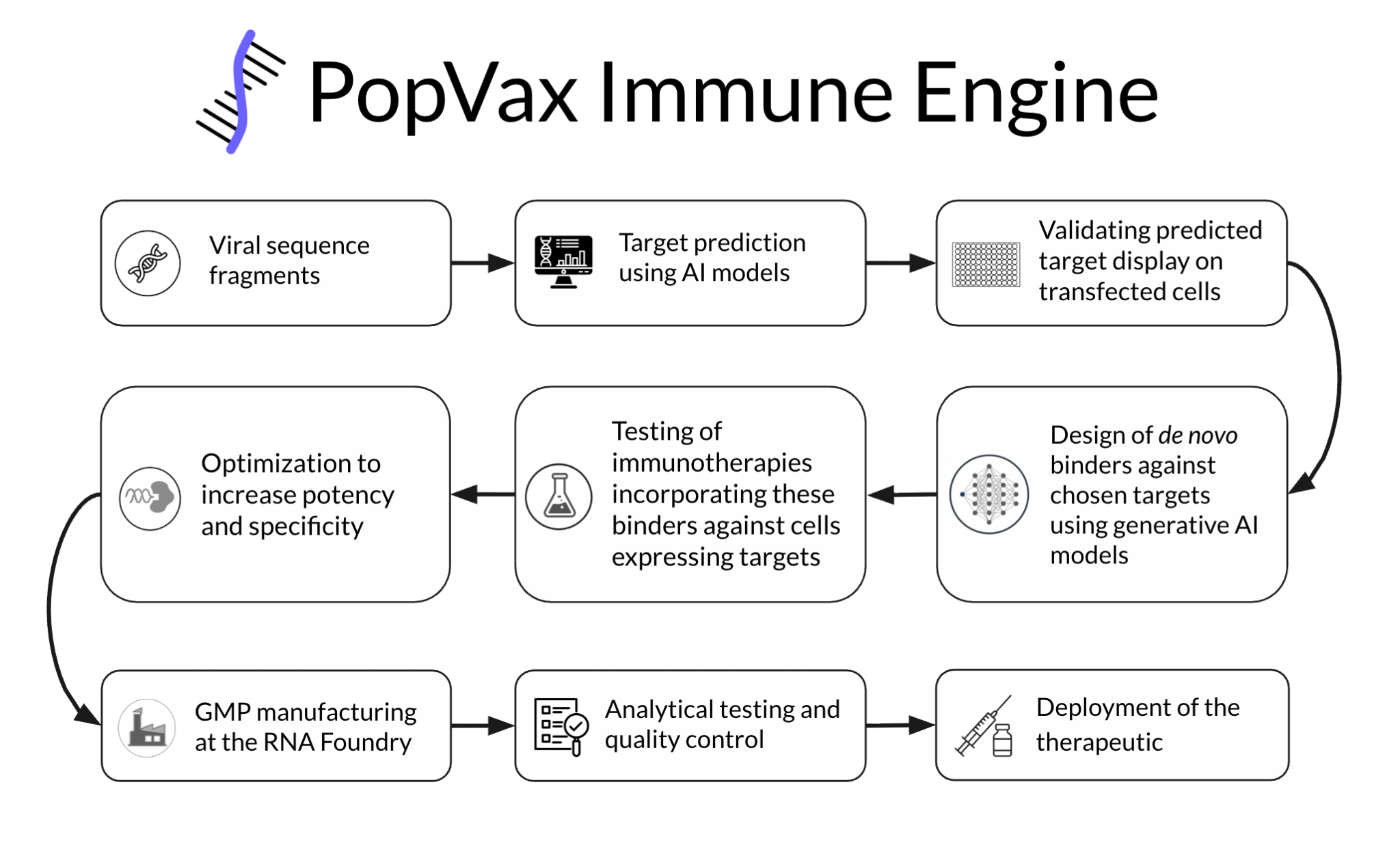
We will implement this capability end-to-end under one roof at our RNA Foundry, integrating:
(a) AI for target epitope identification and design,
(b) high-throughput assays for testing,
(c) rapid translation into a Good Manufacturing Practices (GMP)-compliant production process,
(d) analytical validation and quality control, and
(e) AI fine-tuning and re-training based on in vitro, in vivo, and human clinical trial data to improve candidate hit rate, efficacy, and safety.
The existence of an always-on engine such as this, running hot and ready to rip at all times, would represent a step change in our defense against AI-bio threats. Our ability to treat new infectious diseases would no longer rely on us getting lucky with a novel pathogen that just so happens to come from a viral family for which a lot of R&D has already been done prior to the outbreak, à la coronaviruses and influenza. The end-to-end integration of million-dose manufacturing capacity from day one will help ensure that deployment does not substantially lag development. Our existing RNA Foundry being located next to some of the largest vaccine and biologics producers in the world in Hyderabad already gives us a path to massively ramp up production if and when demand surges during an outbreak or catastrophic biological event.
In the short term, we hope to operationalize and run the Immune Engine end-to-end to design, test, and manufacture therapeutics against an existing understudied pathogen within 12 months as a demonstration, starting with only the viral sequence. We will then take one of these therapeutics into Phase I/II human trials to demonstrate safety. In the medium term, we intend to compress the timeline from design to manufacture down to under 3 months, then 4 weeks, and then even shorter still. In the long term, we intend to design a modular version of the engine that we and our partners can construct in a widely geodistributed fashion across the world. Our upcoming biosecurity operations base in London represents the beginnings of that plan.
The Science Behind the Immune Engine
PopVax has spent the past 4 years using generative AI to develop broadly protective vaccines against COVID-19 and influenza, novel vaccines against difficult pathogens such as HCV, TB (in adults), and Strep A, as well as, over the last year, immunotherapies against deadly diseases like liver cancer and pancreatic cancer.
We are a full-stack biotech built around AI for protein design and our mRNA platform, funded by the Gates Foundation, the US biodefense agency BARDA, and Coefficient Giving/Good Ventures. Our first vaccine program, designed, tested, and manufactured at our integrated RNA Foundry in Hyderabad, is entering a Phase I clinical trial in Australia in just a few months (August 2026).

What this has taught us is that vaccine development is, in fact, very very hard. Our experience demonstrates that current models are superhuman at designing de novo binders to nearly any protein with quite high success rates, but are largely still unable to design effective vaccine immunogens where prior human and classical computational efforts have failed.
Why is this the case? Vaccines are designed to elicit an immune response that then, in turn, neutralizes the pathogen – this second-order nature makes them inherently finicky, and they require biological insight into the target pathogen that is often difficult to glean with just the sequence over the course of a few days. While the COVID-19 vaccines were available faster than antiviral therapeutics, including antibodies, this was enabled in large part by substantial prior work on SARS-CoV-1 and MERS-CoV vaccines, without which development would likely have taken much longer. That effort also relied on the lucky reality that it is indeed possible to rapidly design vaccines against coronaviruses – there are infectious diseases that vaccinologists have been working on for decades, with billions of dollars invested, including HIV, the herpesviruses EBV, HSV, and CMV, and of course HCV, that we don’t have effective vaccines for. This state of affairs persists in large part because we don’t know how to reliably identify or design the right vaccine immunogen to elicit an effective neutralizing response. There are no widely-deployed in vitro or animal models, much less AI models, that can predict whether any given novel vaccine will elicit the right antibodies and T cell responses in humans, let alone be efficacious.
On the other hand, there are multiple classes of therapeutics that boil down to being able to bind to protein antigens on specific cells – these include antibodies, targeted immunotherapies such as bispecific T cell engagers, and cell-specific toxin delivery modalities such as antibody-drug conjugates. Current generative AI models for protein design of the kind that won David Baker a portion of the 2024 Nobel Prize in Chemistry are well set up to enable the development of these therapeutics, providing the ability to generate high-quality binder candidates in minutes and test them in weeks instead of many months.
Indeed, these technologies form a subset of the very same AI architectures and models that have created the biological risks we are working to combat in the first place! The snake eats its own tail, and in the source of our problem lies our potential solution – the Immune Engine builds binding-driven protein therapeutics, in particular targeted immunotherapies such as T cell engagers and antibody-like therapeutics, not vaccines (rest assured, the nominative irony is not lost on us). These therapeutic classes, which are among the leading modalities in cancer immunotherapy, work by simultaneously binding to an immune cell and a specific target cell, forming a bridge that pulls the two cell types into close proximity and triggers the immune cell to kill the target cell.
For our biosecurity use case, we will employ T cell engagers and antibody-like therapeutics to target infected cells displaying a viral protein, or a fragment of a viral protein, on the cell surface, using generative AI to de novo design the proteins that bind to these viral proteins to target the therapeutic towards them. We will use AI to predict targetable proteins and fragments directly from the viral sequence, which would be the only input to the therapeutic design process.
We will particularly target the virus’ critical functional proteins, such as the RNA‐dependent RNA polymerase (RdRP), which in an RNA virus is essential to the ability of the virus to make copies of its own genome for replication. Fragments of the RdRP are likely to be displayed on infected cells via major histocompatibility complex (MHC) molecules, which are a key part of the body’s adaptive immune response, allowing them to be targeted via AI-designed binders as part of a T cell engager or an antibody-like therapeutic to kill the infected cells. Any mutations make the delicate RdRP less likely to function, rendering the virus unviable, which reduces the likelihood of viral mutation rendering the therapeutic obsolete in a short period of time. The RdRP is, of course, just an example – over time, we will train AI to identify essential elements of the viral machinery to target based on predicted function, regardless of resemblance to existing pathogen sequences.
Most viruses infect only a small fraction, typically <1% at peak, of the cells in the human body due to their natural tropism – they favour specific cell types, such as CD4 T cells and macrophages in the case of HIV. It should therefore be possible in many cases to kill off the infected cells in a patient without killing the patient, especially if the infection is caught early enough. It may also be possible to use these medicines as prophylactics, administering them to individuals in at-risk areas to prevent rather than treat infection.
Critically, unlike for vaccines and small-molecule antivirals, testing this kind of therapeutic for indications of efficacy does not require that we have or handle the virus itself. When the labs perform red-teaming exercises around biological capabilities that may result in dangerous outputs, we don’t even need the full sequences of the viruses their models may design to develop therapeutics against them – we can make do with just a few fragments. We can functionally test these T cell engagers and antibody-like therapeutics in vitro by measuring their ability to cause the killing of cells induced to express the target viral protein or fragment, with other healthy cells as a comparison, which is a common approach in cancer therapeutics. This substantially reduces risk while also increasing the speed of development and validation.
T cell engagers in autoimmune and cancer therapy have had issues with immune-related toxicity such as cytokine release syndrome (CRS). This may well prove to be a problem in the infectious disease setting as well, but we believe it is possible to use generative AI fine-tuned on immunological data to mitigate these issues and make these therapeutics considerably safer over time. These side effects are also typically only in evidence when there is a high population of target (in this case infected) cells, so they may not be substantial early in the course of infection or in the prophylactic setting.
In contrast, antibody-like therapeutics, which we can develop using the same methods, use the Fc receptor to engage natural killer (NK) cells and monocytes instead of T cells, and typically have much lower CRS risk, though they can be less effective than T cell engagers.
We plan to manufacture and deliver these medicines using our mRNA platform. mRNA encodes the instructions to make a protein such as a T cell engager or antibody-like therapeutic, not the protein itself, which makes it far easier to manufacture. Unlike a traditional therapeutic protein, which is produced inside living cells maintained in large-scale artificial cultures outside of the body, mRNA is produced in a test tube via in vitro transcription (IVT), an enzymatic, largely cell-free process that makes RNA directly from free nucleotides using a small amount of template DNA made in bacteria. This mRNA is then encapsulated into a lipid nanoparticle (LNP), a fat bubble made from multiple lipid components, in order to allow it to enter into the patient’s cells, which then produce the therapeutic protein themselves, releasing it into the bloodstream to find its target.
RNA is relatively easy to purify, with much less variation in process and yield from sequence to sequence than from protein to protein. This means it is fast and simple to switch out the sequence of the RNA produced by just changing the corresponding sequence in the DNA template used in the reaction. Any issues can be worked out over a few batches over just a few days, rather than over many months for therapeutic protein production in cell culture, enabling our aggressive 4 week timeline to GMP production. The process is also far more compact and scalable – the number of doses worth of RNA we can produce in a 250-litre vat would require many thousands of litres of cell culture in giant floor-to-ceiling tanks.
We’ve already worked extensively on mRNA-encoded T cell engagers for pancreatic and liver cancer, with a particular focus on building the capability to produce personalized cancer therapeutics based on tumour sequencing data from each individual patient within just a few weeks, a timeline enabled by the fact that our GMP manufacturing facility is located just on the other side of the glass from our R&D lab at the RNA Foundry. Sound familiar? The biosecurity therapeutics program we’re proposing draws heavily from our experience and learnings in both infectious disease vaccines and cancer immunotherapies, so we’re very much not starting from scratch, and can spin the Immune Engine up to a hot state very quickly.
Just as with personalized therapeutics, to get timelines for deployment down to weeks from years, we will need to work closely with regulators on accelerated pathways that involve little-to-no clinical testing for new medicines in response to fast-spreading novel viruses. The FDA already has the animal rule, which allows conditional approval for drugs against dangerous diseases that are not actively circulating with only animal (and no human) efficacy studies, and has been used for vaccines and therapeutics against smallpox and anthrax. This sort of pathway would need to be expanded to include novel pathogens that have already begun to circulate, but for which human efficacy studies would take too long.
From our upcoming biosecurity operations base in London, we will work closely with regulators across the world to help build and improve these pathways in parallel with the development of the Immune Engine.
A New Funding Model for Biosecurity
Frontier AI labs are the fastest-growing companies of our time. Anthropic has nearly reached a trillion dollar valuation barely 5 years from its founding, a feat which took Apple, the first company to pull it off, 42 years. The labs openly acknowledge the biological risks their models pose, most recently in a letter signed by the heads of Anthropic, OpenAI, Google DeepMind, Meta AI, and Microsoft AI calling for mandatory DNA synthesis screening. They have put safeguards in place to try and prevent their models from enabling bioterrorists, but by and large have only just begun to articulate plans to halt the advance of an AI-designed virus emerging from their LLMs, or to treat those who fall victim to it.
These companies already conduct red-teaming exercises to catalogue the biological design and assistance capabilities of these models. Results from these demonstrations inform the development of better model safeguards, but could also be used to inform the development of vaccines and therapeutics that combat model capabilities and strategies in pathogen design.
Someone will need to work closely with the labs to build and maintain rapid therapeutic development, manufacturing, and deployment capabilities against the potential outputs of their models as an active defense against biological risk. Leveraging the very tools that create the risk to mitigate it, we must deeply integrate AI into every step of these therapeutic engines in order to allow them to produce effective new medicines to prevent and treat AI-designed viruses in weeks, not years.
Traditional pharma companies are too slow and risk-averse to play this role, and are only moved by financial prospects at a scale that excludes their (early) involvement. In fact, it is exactly this lack of commercial incentives that has made many large pharma companies downsize (Pfizer, Sanofi, GSK, Moderna, BioNTech) and discontinue or divest (J&J, AstraZeneca) their infectious disease programs. This status quo leaves the world dangerously unprepared for the uncapped downside of AI’s biological capabilities. The potentially millions of lives that may be lost in an engineered epidemic should horrify us all, and should particularly alarm the frontier AI labs, who will eventually be held responsible for these consequences if they manifest, just as it should alarm insurers and re-insurers who will have to foot a substantial portion of the bill.
We believe that smaller, nimbler, AI-native teams are the most likely to successfully meet this moment – they are the ones who will build and maintain end-to-end capabilities for rapid response therapeutics against AI-designed viruses. While PopVax, with our full-stack approach, infectious disease expertise, and personalized cancer therapeutics experience, is ideally positioned to develop the Immune Engine, we hope to be only one of many companies working on rapidly available anti-infectives. Operation Warp Speed confirmed the benefit of this diversified approach as well as the importance of startup vigour – of the several vaccines the US government supported, it was unexpectedly the experimental mRNA platforms of the relatively young Moderna and BioNTech that worked best, while Sanofi, GSK, and J&J, the traditional infectious disease giants, largely failed to develop good vaccines.
Biosecurity – just like fire protection and cybersecurity – requires sustained and predictable funding to work. Philanthropic funders like Coefficient Giving, SentinelBio, Renaissance Philanthropy, Founders Pledge, CEPI, and Blueprint Biosecurity have already begun seeding different pieces of the biological resilience puzzle, with the OpenAI Foundation recently joining in. This sort of early funding is essential to help establish technology and infrastructure across the biosecurity stack, but donor money may not be sufficient or reliable enough to keep the engines running hot over the long term – neither is government grant funding, which can be quite fickle as the winds change.
This has been a persistent problem in pandemic preparedness, where funding from both philanthropy and government booms during an outbreak, but collapses soon afterward as that specific threat recedes and the funding becomes politically unpopular. The frontier AI labs, however, have fewer constraints, and should fund always-on capabilities through yearly maintenance and demonstration contracts. These would include continuous end-to-end stress testing with existing understudied pathogens as targets, as well as Phase I/II clinical studies for one or two therapeutics from the Immune Engine and other rapid response therapeutic engines, such as the OpenAI-backed Red Queen Bio, each year for safety and platform validation. Biorisk red teams at the frontier AI labs should further support the improvement of these engines by collaborating with companies like PopVax to provide fragmentary examples of potential threats the models are able to produce, in response to which prototype therapeutics should be rapidly developed and tested.
We at PopVax want to work with one or more of the frontier AI labs to perform a proof of concept demonstration using an existing understudied virus as a target. Our work won’t carry the price tag and timeline of the increasingly obsolete classical pharmaceutical model that takes $2 billion+ and 10+ years to develop each new medicine – we will operationalize the Immune Engine and demonstrate our ability to design, test, and GMP manufacture a new medicine against this virus for under $10M over the course of 12 months. If this goes well, we hope to be able to work out yearly capability contracts that will allow us to accelerate the speed of the Immune Engine, eventually reaching our goal of 4 weeks from viral sequence to manufactured doses, then maintain it and improve it via constant active testing.
In the longer term, we believe that insurers and reinsurers, who will eventually bear much of the private-sector financial burden of an engineered epidemic, will also see value in contractually supporting the Immune Engine.
AI’s biological capabilities have the potential to allow humanity to eradicate the scourge of disease once and for all, ushering in a golden age of health, but they equally have the potential to plunge us into a dark age of de novo viruses and engineered plagues. At PopVax, we believe that it is our bounden duty to harness the power of AI to build active biological defenses that counter the damage that murderers and madmen misusing these tools can cause.
The models are the worst they ever will be at this very moment. If we start building and testing the Immune Engine now, while AI’s biological capabilities are still in their relative infancy, we can keep defense ahead of offense, if only just barely – if we don’t, apocalypse awaits.
Reach out to us at biosecurity [at] popvax.com if you are interested in collaborating with us on combating AI-designed de novo pathogens.
I’m Hannah Herzig, and I lead PopVax’s global biosecurity program out of London. I previously worked for the European Commission, where I helped set up the Health Emergency Preparedness and Response Authority (HERA), and built the team working on diagnostics and medicines for chemical, biological, radiological and nuclear threats. I trained as a physician in Germany, England and South Korea, before completing a master’s degree in public health from Harvard University.
During the COVID-19 pandemic, I volunteered to vaccinate thousands of people at a makeshift clinic in Brussels on my breaks from making policy down the street, which gave me a chance to witness and participate in the pandemic response firsthand from both the bottom up and the top down.
I joined PopVax a few weeks ago because I believe that the tools driving AI-linked biorisks can also be harnessed to protect us from those risks, and that we must start building capabilities like the Immune Engine to help humanity stay one step ahead of infectious diseases.
Email me at hannah [at] popvax.com if you have any questions, comments, or suggestions about this essay or PopVax’s work in biosecurity. You can also find me on Twitter/X @hcherzig.
I wrote this essay together with Soham Sankaran, the founder & CEO of PopVax – you can find him on Twitter/X @sohamsankaran.
You can also follow PopVax on Twitter/X, LinkedIn, and YouTube.
Exciting - the immune engager approach reminds me of Eradivir (similar approach except in small molecule space), which had as far as I remember the best data for therapeutic efficacy late in infection in mice that I'd seen.
Typically (acute) antiviral therapeutics struggle with treating late in infection due to the kinetics of viral infection, but engaging immune cells for killing of infected cells might be a powerful enough mechanism to overcome that!